The year was 2018, and Dr. Gabriel Wardi saw a potential solution to a long-running problem in healthcare: sepsis. Wardi, the medical director for hospital sepsis at UC San Diego Health, says sepsis—an overzealous immune system response to an infection—kills about 10 million people a year worldwide, including 350,000 people in the United States.
Part of the problem with sepsis is that there are a lot of ways it can present, which makes it tricky to diagnose. For years, Wardi had been trying to see if electronic health records could trigger an alert for doctors and nurses when someone becomes at risk.
“Unfortunately, those early alerts were wrong almost all the time, and you can imagine that in a busy hospital, your initial reaction is, ‘Get this thing away from me,’ because it’s wrong all the time, it changes your workflow, and no one likes it,” he says.
But when artificial intelligence entered the scene, Wardi wondered if AI models could more accurately predict who’s going to get sepsis.
“We focused on coming up with a way to pull data out of our emergency department in near real-time, look at about 150 variables, and generate an hourly prediction [for] who’s going to develop sepsis in the next four to six hours,” Wardi says, adding that the resulting deep-learning model is helping save some 50 lives a year at UC San Diego Health.
Across San Diego County, AI is reshaping healthcare. It transcribes audio from appointments and summarizes patient notes. It helps drug companies decode genetic data. It writes draft responses to patient questions. It chats with people with mild cognitive impairments. It even identifies breastfeeding-related conditions from pictures taken with a phone.
All of these enhancements are leading to lasting changes that will dramatically improve medicine, says Dr. Christopher Longhurst, chief medical officer at UC San Diego Health.
“I think the promise is a little overhyped in the next two or three years, but in the next seven to nine years, it’s going to completely change healthcare delivery,” Longhurst adds. “It’s going to be the biggest thing since antibiotics, because it’s going to lift every single doctor to be the best possible doctor and it’s going to empower patients in ways they never have been before.”
These may sound like high ideals, but the money piece of this equation seems to speak to a bright future for AI in healthcare. Investors are taking note of the technology’s promise. According to a recent Rock Health report, a third of the almost $6 billion invested in US digital health startups this year went to companies using AI.
However, all of these innovations come with big questions: Do patients know when AI is being used? Is patient data protected? Will human jobs be replaced? Does anyone really want to talk to a robot about their health? Some worry the technology is progressing so quickly that these concerns will go unaddressed.
“I just hope we don’t get too excited before the technology is really where it needs to be,” says Jillian Tullis, the director of biomedical ethics at University of San Diego. “I’m thinking of Jurassic Park—just because we can do it doesn’t mean we should do it.”
Illustration by Cam Cottrill
The promise—and pitfalls—of AI as a diagnostic tool
Even providers themselves aren’t always keen on utilizing AI programs such as Wardi’s sepsis model.
“Doctors and nurses are usually very, very smart people, and not all of them are going to be excited about having some kind of form of artificial intelligence suggest that someone might be developing sepsis,” Wardi says. “The more senior the physician, the more likely they are not to find value in the model. It could be a generational thing … Younger people are more excited about AI.”
Wardi compares the skepticism around AI to 19th-century physicians’ resistance to the stethoscope. “[Doctors thought] it had no value and would ruin the profession,” he says. “Now, it’s a symbol of medicine.”
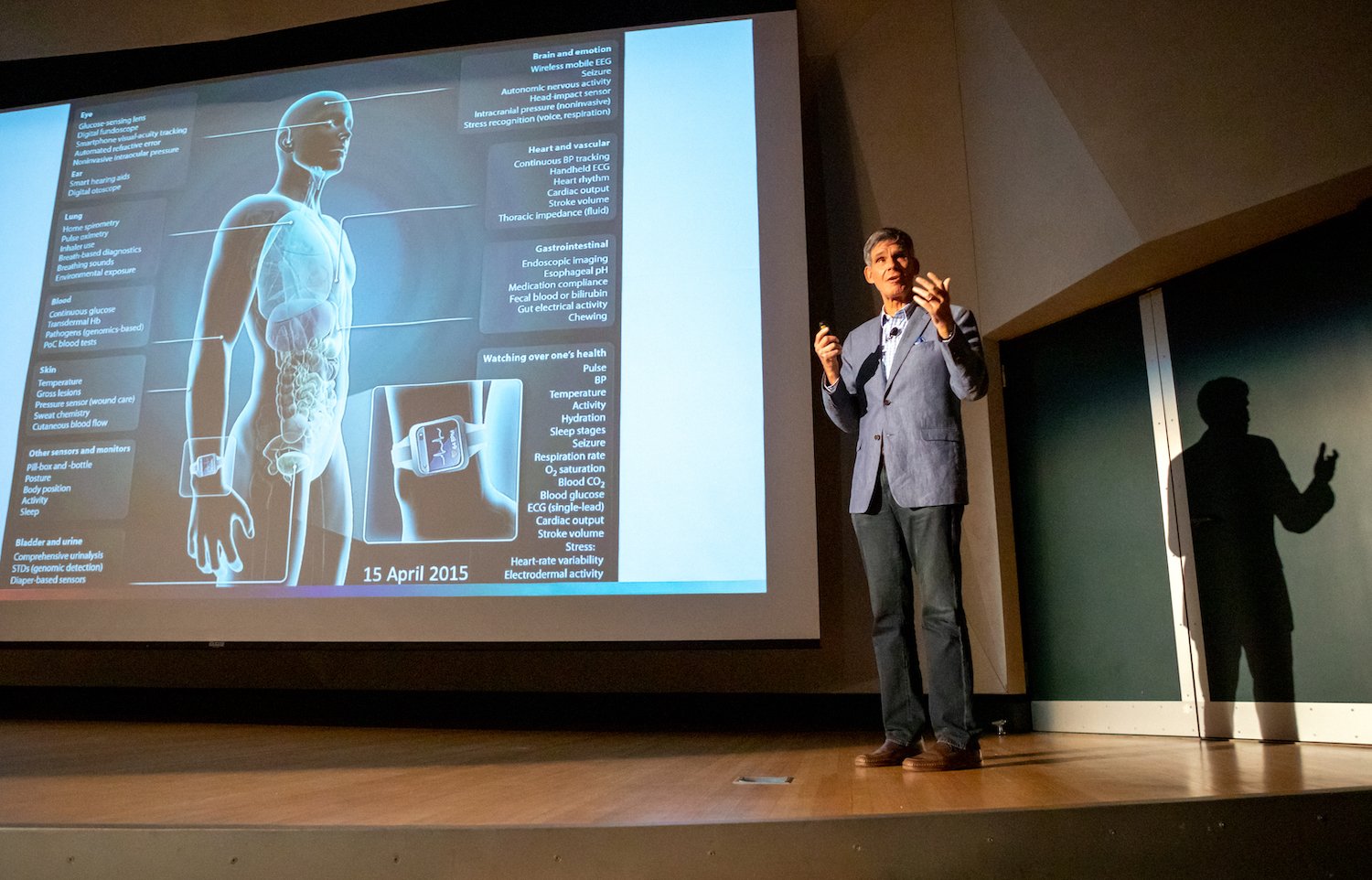
Methods like the sepsis model can be expanded to predict the risk of other diseases, such as cardiovascular conditions, Alzheimer’s, and cancer, says Dr. Eric Topol, director and founder of the Scripps Research Translational Institute.
Courtesy of Scripps Research
“So we take all of a person’s data—that includes their electronic health record, their lab tests, their scans, their genome, their gut microbiome, [and their] sensor data, environmental data, and social determinant data,” he explains. “We can fold that all together and be able to very precisely say this person is at high risk for this particular condition.”
According to Topol, Scripps researchers are even using pictures of the retina to predict Alzheimer’s and Parkinson’s years before any symptoms show up. “Machine eyes or digital eyes can see things that humans will never see,” Topol adds.
Meanwhile, at the San Diego biotech company Illumina, researchers are using an algorithm to analyze genetic information and find mutations that cause disease.
But creating this type of intelligence is a challenge compared to building programs like ChatGPT, which train on data from the internet. Dr. Kyle Farh, VP of Illumina’s Artificial Intelligence Lab, has turned to primates, sequencing their DNA and using that data to train the company’s model, PrimateAI-3D. He hopes to one day use the model to diagnose rare genetic diseases.
Tullis at USD says she’s all for predicting and preventing illness, but she’s worried about the other uses of AI.
“When I read stories about doctors who are fighting with insurance companies about whether or not patients should get certain procedures or treatment, but the insurance company uses an algorithm to make a determination… I get really nervous,” she says.
Diagnosis often requires a human touch, she adds.
“You can look at people’s nail beds; you can look at lumps or rashes in particular ways; you can feel people’s skin if it’s clammy and cold,” she says. “The algorithm can’t do that.”
Illustration by Cam Cottrill
Saving time while protecting patient data
Anyone who’s used an AI model to draft an email or write a cover letter knows it can save a massive amount of time. And doctors and nurses in San Diego are already utilizing AI to take care of some of their more menial tasks.
Several health systems, including Scripps Health, use AI to generate post-exam notes, answer patient questions, and summarize clinical appointments. It can reduce documentation time to “about seven to 10 seconds,” says Shane Thielman, chief information officer at Scripps. “It’s enabled certain physicians to be able to see additional patients in the course of a given shift or day.”
Courtesy of UC San Diego Health
UCSD uses a similar system. According to Longhurst, it’s freed doctors up to focus on patients—not computer screens—during appointments.
“That’s really about rehumanizing the exam room experience,” he says. Since they don’t have to take notes, physicians can make eye contact with patients while the tech transcribes their conversations.
But the approach raises concerns about consent and data privacy. Jeeyun (Sophia) Baik, an assistant professor who researches communication technology at University of San Diego, recently studied loopholes in federal HIPAA law that health data can fall into.
HIPAA does not currently protect health data collected by things like fitness apps or Apple Watches, she says. And that legislative gap “could apply to any emerging use cases of AI in the areas of medicine and healthcare, as well,” Baik adds.
For example, if physicians want to utilize protected health data for any purpose beyond providing healthcare services directly to the patient, they’re supposed to get the patient’s authorization. But it’s debatable whether that applies if healthcare providers start to use the information to train artificial intelligence.
“It can be controversial, in some cases, whether the use of AI aligns with the original purpose of healthcare service provisions the patients initially agreed to,” Baik says. “So there are definitely some gray areas that would merit further clarification and regulations or guidelines from the government.”
A recent California state bill, SB 1120, attempts to clear up those gray areas by requiring health insurers that use artificial intelligence to ensure the tool meets specified safety and equity criteria.
Thielman with Scripps Health says patients must always give consent before the AI tool takes notes on appointments. If a patient declines, providers won’t use the technology. However, “it happens very rarely that we have a patient that doesn’t consent,” he adds.
And, he continues, a human always looks over automated, AI-generated messages answering patient questions. But Scripps doesn’t tell patients that it’s using AI “because we have an appropriate member of the care team doing a formal review and signing off before they release the note,” he says.
It’s the same case at UCSD.
“There’s no button that says, ‘Just send [the message to the patient] now,’” Longhurst explains. “You have to edit the draft if you’re going to use the AI-generated draft. That’s adhering to our principle of accountability.”
Jon McManus, chief data, AI and development officer for Sharp HealthCare, says he realized an internal AI model was necessary to ensure employees and providers didn’t accidentally input patient data into less secure algorithms like ChatGPT. “We were able to block most commercial AI websites from the Sharp Network,” he explains. Instead, his team created a program called SharpAI. It’s used for tasks like summarizing meeting minutes, creating training curriculum, and drafting proposed nutrition plans.
Fixing mistakes—and possibly making them
With artificial intelligence technology, telehealth services could get way more advanced—Jessica de Souza, a graduate student in electrical and computer engineering at UCSD, is currently working on a system that would allow parents experiencing breastfeeding problems to send photos of their breasts to lactation consultants, who could use AI to diagnose what’s wrong. De Souza created a dataset of breast diseases and trained AI to identify patterns that could indicate issues such as nipple trauma.
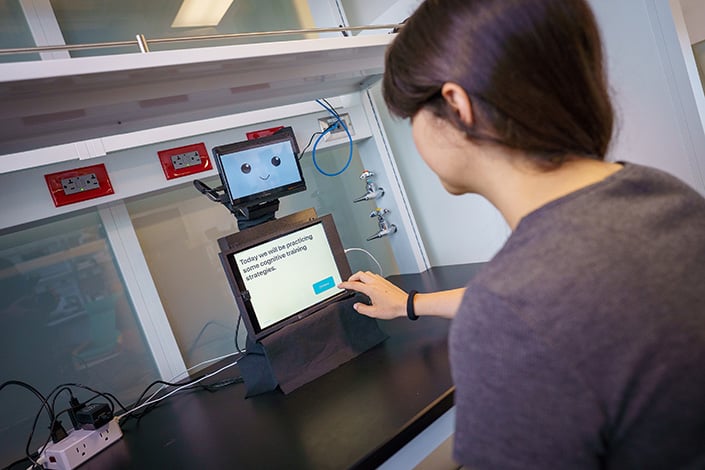
Meanwhile, Laurel Riek, a computer science professor at UCSD, designed a small, tabletop robot called “Cognitively Assistive Robot for Motivation and Neurorehabilitation,” or CARMEN (the name is inspired by Carmen San Diego). CARMEN helps people with mild cognitive impairment improve memory and attention and learn skills to better function at home.
Courtesy of UCSD
“Many [patients] were not able to access care,” she says. “The idea behind CARMEN is that it could help transfer practices from the clinic into the home.”
Uses like these offer another vision for AI in healthcare: to improve patient care by helping doctors assess conditions and find mistakes.
“One of the big things is getting rid of medical errors, which are prevalent,” Topol says. “Each year in the United States, there are 12 million diagnostic medical errors.” According to Topol, those errors cause serious, disabling conditions or death for about 800,000 Americans per year.
He believes that AI can help shrink that number considerably. For example, doctors are utilizing it to review cardiograms, checking if there’s anything a human review missed.
But, Topol cautions, you can’t rely solely on AI. “In anything involving a patient, you don’t want to have the AI promote errors,” he says. “That’s the thing we’re trying to get rid of. So that’s why a human in [the] loop is so important. You don’t let the AI do things on its own. You just integrate that with the oversight of a nurse, doctor, [or] clinician.”
No matter how advanced artificial intelligence programs get, he sees no future where AI would handle diagnosis without human eyes.
“You don’t want to flub that up,” he says. “And patients should demand it.”
Algorithmic bias
An additional hope for AI is that it could correct for implicit racism in medicine, since machines, in theory, don’t see skin color. But the data on which algorithms are built is inherently imperfect.
“The medical bias could be already built into the existing information that’s out there,” Tullis says. “And, if you’re drawing from that information, then the bias is still there. I think that’s a work in progress.”
For example, an AI tool designed to detect breast cancer risk would be trained on previously gathered population data. “But they didn’t get as many Black women as they would like to be included in that data,” Tullis explains. “And then what does that mean for the quality of the data that has been used to maybe make decisions?”
Courtesy of Scripps Research
But there’s bias in every data set, Longhurst says. The key is to choose the right data for the population you’re working with to help address disparities. He points back to the sepsis model. That algorithm, he says, actually performed far better in UCSD’s Hillcrest hospital than in La Jolla.
“Why is that? Well, we tuned the algorithm to identify cases of sepsis that weren’t being picked up [by physicians] until later,” he adds. “We serve different populations in those different emergency departments.”
Patients at the Hillcrest location tend to be younger, which makes it harder to diagnose sepsis early, he says. But the AI algorithm helped to close that gap.
“These tools are going to change healthcare delivery more in the next 10 years than healthcare has changed in the last 50,” Longhurst says. But he hopes the industry doesn’t get ahead of itself—after all, he suggests, what if the FDA approved a new drug for breast cancer and simply said, “It has very few side effects?”
“You’re like, ‘Well, that’s great, but how does it work?’ They’re like, ‘Well, we don’t really know. We don’t have the data,’” he continues. “That’s what’s going on now. It’s like the Wild West. Our argument is that we really need local testing that is focused on real outcomes that matter to patients. That’s it.”
Claire Trageser has been writing for San Diego Magazine for 10 years. She also is a reporter at KPBS and writes for The New York Times, National Geographic, Marie Claire, Elle and Runner's World.
Before, during, and after the Fourth of July, San Diegans can commemorate America’s 250th anniversary with an abundance of stars, stripes and local celebrations. America The Beautiful: 250 at The Rady Shell and Lamb’s Players Theatre’s revival of American Rhythm will look back at the many songs which define our country. Liberty Station’s Anchored in Freedom celebration and the Independence Day Carnival offer community-centered fun and loads of family-friendly activities. And who can possibly forget the Big Bay Boom, which will resume its reign over San Diego Bay as the state’s biggest fireworks show. Outside of the holiday festivities, this week brings the yearly return of Little Italy’s Summer Sera and the Athenaeum Summer Festival, as well as a slate of championship matches for All Elite Wrestling.
Sip on refreshing beverages and savor a panoramic rooftop view this Friday from 6-8 p.m. during the 21-plus Sunset & Spritz at Margaritaville Hotel San Diego Gaslamp Quarter’s 5 O’Clock Somewhere Bar. There will be a live DJ (until 9 p.m.), appetizers, pool and cabana access, a photo booth, and a cash bar (until 11 p.m.). To accentuate the summer theme, guests are invited to dress in white, pink, and orange attire. Tickets are $29 and come with a welcome aperol spritz.
616 J Street, Gaslamp
The 250 Grand Tasting Menu at Amaya
July 3 & 4
Bring a patriotic palette to the Fairmont Grand Del Mar for The 250 Grand Tasting Menu at Amaya this Friday and Saturday from 5-8:30 p.m. Patrons will be treated to a five-course tasting menu, curated to exhibit a selection of standout regional flavors and culinary concepts that have shaped our country’s distinct food heritage. The meal will also include beverage pairings with each course, such as wine, cocktails, and artisanal drinks. Reservations are $330 per person (with tax and 20% gratuity) on OpenTable.
Don Toliver thrives at being the life of the party (and the “After Party”). His fifth album Octane, released in February, is indicative of his thrill-seeking nature. As with his earlier releases, Octane sees Toliver operating in the space between hip-hop and R&B, with warbling vocals and blaring beats that are best heard at a high volume. This Tuesday at 7:30 p.m., Toliver will play at Pechanga Arena, with rappers SoFaygo, Chase B and SahBabii—who had a guest verse on Octane standout “K9”—as special guests. Tickets start at $156 for this concert.
What makes musicals like Wicked, Cats, Chicago, and Jersey Boys so timeless is the legion of excellent songs that makes fans out of those who’ve never even watched the show. This Friday at 7:30 p.m. during Blockbuster Broadway! at The Rady Shell, conductor Evan Roider, the San Diego Symphony Orchestra, and veteran vocalists Alex Getlin, Jessica Hendy, Scott Coulter, and John Boswell (also on piano) will perform an all-star theater soundtrack. In addition to the shows named above, audiences can expect songs from A Chorus Line, The Phantom of the Opera, Annie,and more. Tickets range from $57 to $129 for this concert.
222 Marina Park Way, Embarcadero
America The Beautiful: 250 at The Rady Shell
July 4
One night after recognizing the brilliance of Broadway, The Rady Shell will ring in the United States’ landmark anniversary with America The Beautiful: 250 this Saturday at 7:30 p.m. Conductor Byron Stripling, joined by a five-performer ensemble and the San Diego Symphony Orchestra, will lead a night of ballads that best resemble the red, white, and blue, including songs sourced from the Great American Songbook. After the show, concertgoers are invited to watch the nearby Big Bay Boom from their seats. Tickets range from $71 to $139 for this concert.
222 Marina Park Way, Embarcadero
Athenaeum Summer Festival at Athenaeum Music & Arts Library
Ryan Hardison is a freelance arts and entertainment writer and recent graduate of San Diego State. When he's not staring at his laptop, he's likely eating an adobada burrito or getting sunburnt at the beach.
“This is insane!” the guy filming it seems to proclaim. “It’s the best fireworks show ever!” a companion confirms, inspiring a debate lasting over a decade.
All told, 7,000 fireworks exploded in the span of 25 seconds over San Diego Bay on July 4, 2012. A Michael Bay amount of unison. $125,000 worth of shells, cakes, Roman candles, and skyrockets had been placed on a barge—enough for 17 minutes of decorative sky flares—and…
Boom.
The sky looked like someone had set a giant Rorschach test on fire. Or as if whatever we all see in our Rorschachs—butterflies, clowns, tongue kissing, dads—was being electrocuted and lifted heavenward, amen. It was shocking how bright it was, how much it sizzled the local cosmos. Could’ve been one of those sci-fi films where a hole is ripped open between warring universes. But angstier, more metal—the work of some methy creator in a sleeveless concert tee.
The sound?
Lou Reed once released an entire album that contained 64 minutes of mindflaying guitar screeches and machine noises. No regular songs, just a fascinating amount of ear distress. His record label reps no doubt heard the melodic outro of their careers, but everyone else was in pain and stumped. That album still sounded better than the bay did that night. The bay sounded like a god who struggled with emotional regulation had blown his speakers and was working through the anger stage of AV grief.
In the left frame of the video, a middle-aged woman is attempting to drag her husband off by the hand. In no way does he want to go, possibly because he had missed the time Roseanne Barr sung the national anthem at a Padres game, simultaneously disemboweling and amusing America through the power of song. He would not willingly abandon an equally worthy San Diego trainwreck.
Another woman in the video appears to have just filled her beer, rushing to sit down for the show. She pauses mid-sit and returns to the full and upright position to properly bear witness. What was supposed to be prolonged entertainment has been so radically shortened that she will have to find another reason to drink. Lucky for her, drinking will be the only way to adequately process.
Locals remember the conspiracy theories. People wondered if the fuses had been tripped by a saboteur who was sympathetic to dogs, fish, or the growing suspicion that late-stage capitalism is a gorgeously branded but impossible dream sustained by remarkably efficient top-tier wealth retention and the soft compliance of fireworks-watchers who can no longer afford a house, a beer, or the personal impacts of human reproduction.
Speaking of being terrified of babies, babies were terrified. The children who witnessed it probably still can’t go near a candle store. But those kids will be tougher, perfectly scarred kids. They’ll write better songs.
That night helped us absolutely dominate the national news cycle. For a hot minute, we became America’s water-skiing squirrel. Now, years later, when you Google “fireworks gone wrong,” San Diego is always a top contender, along with that poor Nebraska family who nearly wiped out a couple generations in their front yard, their minivan somehow turning into a howitzer of recreational TNT.
There is still debate as to whether Big Bay Boom 2012 is the worst or greatest fireworks show of all time. But the advanced parts of civilization arrived at the truth as quickly as the women in the video did. It was undeniably amazing.
First of all, the point of Fourth of July fireworks isn’t “the intricate choreography of sky fire over a guaranteed amount of show time.” It’s about creating a vivid memory shared with some people you like, love, or would like to love.
BBB2012 used large-scale chemical fire to create the ultimate memory.
Sure, some people who iron their jeans subjected their family to a sermon about how San Diego managed to botch America’s birthday like a Disney princess-for-hire who smelled of quite a few Sauvignons.
The rest of us saw how perfectly it nailed the actual feeling of being an American. Because only a miniscule percentage of us bake postcard apple pies where every inch of crust is perfectly laminated like the wood in an Irish bar. Very few of us can paint on par with Picasso. The rest of us—despite truly believing in our America-activated abilities to achieve greatness in almost any field of our choosing—burn pies. We try to paint only to realize it looks like our fine motor skills have entered active death.
That’s why BBB2012 was the most perfectly American fireworks show ever: A wildly ambitious idea galvanized thousands upon thousands of people to both work on it and come to hold a beer and gawk at it, only to have it fail in the most glorious TMZ-level spectacle.
America isn’t about immaculate, storyless wins. It’s about how the framework of a country is solid enough that we can accidentally detonate our entire lives—a few times—and still probably be OK.
No one has America’d quite like San Diego did on that day. It was performance art. Lou Reed’s heart slow-clapped. Any brief municipal embarrassment quickly became a pride of our people. I can only hope the same for the Nebraskan yard family whose Dodge Aerostar became a hyperactive Death Star.
P.S. Local writer Maya Kroth compiled a quite great oral history of that night for Thrillist. The bottom lines for me were—it took nine months to prepare, no one was hurt, and even though the pyrotechnics company tried to zero out the bill, Big Bay Boom founder H. P. “Sandy” Purdon refused and paid them in full. This year will mark the 25th Anniversary of the yearly Big Bay Boom.
Troy Johnson is the magazine’s award-winning food writer and humorist, and a long-standing expert on Food Network. His work has been featured on NatGeo, Travel Channel, NPR, and in Food Matters, a textbook of the best American food writing.
If absence makes hearts (and stomachs) grow fonder, then shuttered restaurants quickly become the hottest tickets in town—something a number of iconic institutions found out after taking very public hiatuses after historically long runs. For instance, following a lengthy (and extremely flip-floppy) closing process after 92 years in business, Las Cuatro Milpas reopened two blocks away in Mercado del Barrio. Similarly, Carlsbad butcher shop Tip Top Meats reopened in the same location (albeit a smaller space) after the death of founder Joachim “Big John” Haedrich in 2023. Finally, after a whopping decade out of business, Sami Ladeki and chef Alfie Szeprethy brought back Roppongi to its original Prospect Street space, where it was the talk of the town in the late ’90s. All came back under the same proprietors, so they weren’t third-party nostalgia-licensing deals. The algorithm may have ravaged our attention spans away from all but the newest and shiniest, but this proves there’s still hope for our collective prefrontal cortex.
Other local eateries honored their pasts by bringing in new perspectives. The Lion’s Share in Embarcadero, Milton’s Deli in Del Mar, Dudley’s Bakery in Santa Ysabel, and J-K’s Greek Cafe in La Mesa handed over the keys to new owners willing to take on a big task: maintain the soul of icons through particularly rough economic circumstances for restaurants, navigate big feelings from longtime regulars (who often don’t take kindly to change), and make some necessary changes to keep going for another few decades. Taking over a project in process can be a lot harder than starting from scratch. But building that feel-good nostalgia doesn’t happen overnight, so it sure helps to have a well-established playbook of success passed down from those who came before.
Courtesy of Sugarfish
The Expansion Class Arrives
It wasn’t just restaurant groups from Los Angeles that decided to put down roots en masse, although San Diego saw plenty of LA transplants recently (Sugarfish, Mr. Charlie’s, For the Win, Katsuya Ko, Bacari). Global brands like Chef Fei, Zuma, and Pepper Lunch have locations of their own on the way, and upscale Canadian eatery Joey joined to the inescapable gravitational pull of Westfield UTC’s culinary cosmos for its first spot in America’s Finest City. Good to see the rest of the world is catching up with what we’ve been seeing the last few years—San Diego is a dining destination already on the rise.
Choosing To Not Choose
Between the never-ending news cycle of doom and perimenopause brain fog, I’m at the stage in life where I’m more than happy to let someone else make a decision for me, especially when it comes to what’s for dinner. And based on the way a lot of menus look right now, I’m not alone. It seems like half the places I visit offer some version of a prix fixe, omakase, or tasting menu. Restaurants are embracing the curated experience to solve the problem of affordability (a fixed menu reduces food and labor costs, guarantees an acceptable check average, etc.) and critical thinking in one fell swoop. Omakase (meaning “I leave it up to you”) is far from a new concept in high-end Japanese sushi culture, but now that it’s popping up everywhere from coffee experiences to grab-and-go sushi and sandwiches, it’s gone from somewhat niche to nearly omnipresent.
Courtesy of Rikka Fika
Local Coffee Hit the World Stage
The world got an up-close look at San Diego’s coffee industry when we hosted the premier specialty coffee expo World of Coffee for the first time this April. San Diego’s long and rich coffee history stretches back to the late 19th century. Things percolated fairly quietly for around a century before really picking up steam. Today, there are nearly 200 specialty roasters and cafes across the county, with many earning national accolades like the Good Food Award (Steady State Roasting, 2020; Bird Rock Coffee Roasters, 2023, 2021, 2019, 2017, 2016), Roaster of the Year by Roast Magazine (Mostra Coffee, 2020; Bird Rock Coffee Roasters, 2012), and the Specialty Coffee Association Coffee Design Award for packaging (Rikka Fika, 2026). Now that we’ve moved past the comically insufferable coffee snob era of the early 2000s, even java newbies can feel comfortable walking into pretty much any coffee shop in San Diego, asking questions, trying a few things, and feeling confident they’re going to get great service and a great beverage.
Beth Demmon is an award-winning writer and podcaster whose work regularly appears in national outlets and San Diego Magazine. Her first book, The Beer Lover's Guide to Cider, is now available. Find out more on bethdemmon.com.
Kelly H. Harfouche, founder of KQ Aesthetic Society, knows firsthand that cosmetic treatments like fillers, neurotoxins, and microneedling, can not only enhance a person’s appearance and restore confidence, they have the power to truly change a person’s life. An expert injector has the ability to tailor treatments to each individual patient’s anatomy and goals for personalized results. Harfouche, a board-certified nurse practitioner, has spent nearly a decade perfecting her craft as an aesthetic injector and integrating her multifaceted artistic skills with precision patient care. Her commitment to continual education and training, plus a passion for helping people look—and feel—their best, set KQ Aesthetic Society apart in a sea of local medspas.
For many people considering nonsurgical treatments, the intent is to look refreshed and refined. KQ Aesthetic Society’s philosophy eschews a cookie cutter approach that bases treatments around units, instead working to understand each person’s unique goals, then curating a treatment plan to fit that vision. Harfouche focuses on “inclusive luxury,” the belief that everyone deserves access to aesthetic treatments, respective of budget restrictions. She develops long-standing trusted relationships with her patients, and works with each one to achieve their aesthetic objectives and address the underlying causes of their concerns.
“For me, forming an honest and open relationship with every patient who walks through the door is essential. This means understanding them on a deeper level and meeting them where they are to define and achieve their individual goals,” she says.
Drawing on her artistic background, which inspired her transition into medical aesthetics, Harfouche sees each client as a “unique canvas.” Rather than relying on standardized procedures, the practitioner’s distinctive approach combines her profound understanding of the physiological and anatomical changes associated with aging with an unwavering commitment to ongoing education about the newest products and their mechanisms of action. Her goal is to make each patient feel beautiful in their own skin and to embrace their individuality.
She has also pioneered a way to combine her talent for aesthetic artistry with her philanthropic nature. Harfouche is one of only a handful of providers using dermal fillers to treat patients with lip asymmetry and scarring resulting from cleft lip surgery. Patients travel from around the country for this transformative treatment, noting increased confidence and a restored identity. She hopes to eventually launch a training program to help fill the void in this space.
“My passion has always been connecting with people and giving back in any capacity that I can,” she says. In the rapidly advancing landscape of aesthetic medicine, you can place your confidence in Harfouche and KQ Aesthetic Society to deliver exceptional care. To learn more or book a consultation, please visit kqaestheticsociety.com.
Summer has officially kicked off, and San Diego is celebrating the sunny season with a myriad of fun events. From San Diego Pride week and a fairytale performance at Civic Theatre to a Santigold concert and Comic-Con, there are dozens of opportunities to make memories worth adding to your scrapbook. Here are all the best things to do in San Diego this July:
Divine inspirations, operatic ballads, and symphonic pop production elevate Rosalía’s Lux to heavenly levels. Hear angelic vocals ascend—in up to 13 languages—during her performance at Pechanga Arena.
Enjoy a night of feel-good indie rock and sing-along anthems at the Cal Coast Credit Union Open Air Theatre courtesy of Young the Giant and special guest Cold War Kids.
29
Santigold collects genres like gold stars: musical accouterments that brighten her uniquely alternative sound. See her live in concert with dancehall producer Troy Baker Sound at Humphreys Concerts by the Bay.
Two male government workers pursue a secret romance amid the Lavender Scare in the San Diego Opera’s production of “Fellow Travelers” at the Balboa Theatre.
Audrey Hepburn. Marlon Brando. Salvador Dalí. What do these icons have in common? Each was the enigmatic focus of a Cecil Beaton portrait. Step inside Cecil Beaton’s Fashionable World, an alluring showcase of 20th-century style at San Diego Museum of Art.
Courtesy of San Diego Pride
More Fun Things to Do in San Diego This Month
1
The Little Italy Mercato will trade morning rays for golden-hour glow through its free Summer Sera, an expansion of the neighborhood’s farmers market with live music, artisanal finds, and a fetching amount of pet activities.
11–19
San Diego Pride week starts with a Dyke March and ends with the two-day “Pride Shines On” festival. The days in between? Run a 5K, march in the parade, visit the rainbow-lit St. Paul’s Episcopal Cathedral, and more.
19
Dress up for a Mediterranean-themed tea time at the Estancia La Jolla, a laid-back yet refined afternoon planned for the resort’s monthly Tea in the Garden series.
23–26
Nerd culture’s biggest gathering returns to the Convention Center. San Diego Comic-Con welcomes fans of everything from comic book cinema to ultra-rare collectibles for panels, exhibits, sneak peeks, and much more.
Ryan Hardison is a freelance arts and entertainment writer and recent graduate of San Diego State. When he's not staring at his laptop, he's likely eating an adobada burrito or getting sunburnt at the beach.
You’re coasting home after a weekend in Rosarito Beach—still riding the high of vitamin D and Baja Med—and then comes a slap back into reality: brakelights and gridlock exhaust.
Small wonder, given that San Ysidro is the busiest land border crossing in the western hemisphere (fourth-busiest in the world). Otay Mesa’s no breeze either; it’s the busiest commercial port in California and second-busiest across the entire southern border. Smart Border Coalition says that each day last year, 41,800 vehicles crossed into the US at San Ysidro; 17,800 crossed at Otay Mesa, along with 1,023,000 commercial trucks.
Diana Pazos, a San Diego resident and adolescent psychiatrist working in Tijuana, says the northbound border wait at the San Ysidro crossing is often three to five hours Saturday through Monday—delays that modern humans and multinational maquiladoras alike aren’t built to endure. At the current Otay crossing, “commercial trucks may be in line for six hours or longer,” she says.
Needing to bake a couple hours of commute into the States doesn’t just affect vacations; tens of thousands of people cross the border each day for doctor’s appointments, work, school, you name it. The clog has personal and commercial ramifications.
But change is coming. Construction has begun on a new border crossing in Otay Mesa, which is expected to significantly reduce wait times across all San Diego border crossings, bolster binational trade, and improve the air pollution levels in the area.
Nikki Tiongco, an 18-year Caltrans veteran who oversees the Otay Mesa East project (aka Otay 2) for the agency, says the new border crossing will also be among the most high-tech, efficient, and secure border crossings in the nation.
“We have already completed the roadway network within the Otay Mesa East region,” says Tiongco. Part of this project included building State Route 11, an extension of SR 905, which has been open to the public since August and will feed traffic to the new entry port. Otay 2 comes with a 21st century upgrade, too. Miles of fiber-optic cables have been installed underground, which gives the port the brainpower to efficiently sort and streamline traffic as cars approach the border. (Unlike the San Ysidro border, where lanes get organized by vehicle type, Otay 2’s lanes will be interchangeable. For example, if the system indicates that a high number of commercial trucks is heading to the border, passenger lanes could be converted to cargo lanes in real time.)
Otay 2, driven by a binational collaboration among government agencies (Caltrans, SANDAG, General Services Administration, and U.S. Customs and Border Protection), receives both federal and state funding, plus hefty contributions from Mexico. So far, funds from the $1.3 billion project have helped build new bridges and roadway interchanges that will guide traffic to the crossing. At this stage in the process, Caltrans is “laser-focused on building the facility itself,” Tiongco says.
Now, to the juicy part: the prospect of a “20-to-30-minute border wait time” at Otay 2, according to Tiongco. Currently, there are three standard ways to cross the border at San Ysidro: Ready Lanes, General Lanes, or SENTRI Lanes. Most travelers use either the Ready or General lanes. SENTRI Lanes require a form of pre-approval from the US federal government plus an additional fee. According to CBP, the average wait time in 2025 at the San Ysidro crossing, was as little as 15 minutes in the SENTRI Lanes, 45 minutes in the Ready Lanes, and 1.5 to 2 hours in the General Lanes. Those are best-case scenarios that vary based on lane type and time of day.
Otay 2 is about 12 miles east of the San Ysidro crossing and 2.5 miles east of Otay 1. Those not wanting to spend that much extra time on the road to drive to the new border crossing, despite the allure of an under-30-minute wait, are still expected to see some benefits. Tiongco says Otay 2 will “provide a relief valve” overall by spreading the burden across the three border crossings. As a result, SANDAG says, wait times at San Ysidro and Otay 1 could be cut in half.
It’s not just your time waiting at the border that matters. Multinational corporations that relocated their manufacturing plants (maquiladoras) to Northern Baja have claimed for years that the long delays at Otay 1 eat away at their profits. More than 600 maquiladoras, used by companies such as Samsung and Panasonic, currently use Otay 1 to transport products to US and international markets. Ambassador Alicia G. Kerber-Palma, the consul general of Mexico in San Diego, says the project will facilitate more than $60 billion in cross-border trade annually.
Previous reports say that Otay 2 also has the capacity for around 12,000 passenger cars and 1,500 commercial trucks daily. A shiny, new element to this port: Commercial and personal vehicles that choose to cross will pay a dynamic toll on both sides of the border. The fee will increase during busy hours and decrease during slower periods, Tiongco says. Caltrans estimates that the toll could range from $4 to $30 for passenger vehicles and higher for commercial trucks. Drivers will be able to see current rates before they reach the actual border crossing.
And, with these changes, there are environmental benefits, too. “With shorter wait times at all three ports, there’s less idling and congestion, which should significantly reduce air pollution on both sides of the border,” says Kerber-Palma. The main factor driving improved air quality would be decreasing dirty emissions from idling diesel trucks. This county’s air could use some sprucing up, anyway. A 2026 report from the American Lung Association named San Diego as the fifth-most particle-polluted county in the US. The bulk of that dirty air comes from the heavy-duty trucks and ships that pass through the area.
Otay 2 is not only expected to curb the acceleration of air pollution in San Diego; if the state’s legislature passes California Senate Bill 10, the border crossing could also restore local water quality. This bill would use a portion of Otay 2 toll revenues to fund ongoing maintenance of the South Bay International Wastewater Treatment Plant. Current media reports say, however, that it’s increasingly unlikely that SB 10 will become law.
Otay 2 has been in the works for over two decades and is finally nearing the finish line. Construction estimates show that it should be up and running in 2029. Tiongco says this border crossing is “a good example of how the state, federal and local governments are working together and with Mexico to advance our mutual goals in the region.”
AVRP Studios’ tradition for Design Excellence and Innovation began in 1976 with Doug Austin, FAIA, in Solana Beach, California. The firm has since grown to complete major projects throughout the United States and Canada. We think of ourselves as a family and we care deeply about people. We want to inspire, help make their lives richer and more complete through our efforts. We believe that architecture is one of the most important art forms because of the impact it can have on the lives of those it touches. We’re delighted to have been recognized with over 150 awards for design excellence.
703 16th Street, Suite 200, San Diego, California 92101 | 619-704-2700 | avrpstudios.com