The year was 2018, and Dr. Gabriel Wardi saw a potential solution to a long-running problem in healthcare: sepsis. Wardi, the medical director for hospital sepsis at UC San Diego Health, says sepsis—an overzealous immune system response to an infection—kills about 10 million people a year worldwide, including 350,000 people in the United States.
Part of the problem with sepsis is that there are a lot of ways it can present, which makes it tricky to diagnose. For years, Wardi had been trying to see if electronic health records could trigger an alert for doctors and nurses when someone becomes at risk.
“Unfortunately, those early alerts were wrong almost all the time, and you can imagine that in a busy hospital, your initial reaction is, ‘Get this thing away from me,’ because it’s wrong all the time, it changes your workflow, and no one likes it,” he says.
But when artificial intelligence entered the scene, Wardi wondered if AI models could more accurately predict who’s going to get sepsis.
“We focused on coming up with a way to pull data out of our emergency department in near real-time, look at about 150 variables, and generate an hourly prediction [for] who’s going to develop sepsis in the next four to six hours,” Wardi says, adding that the resulting deep-learning model is helping save some 50 lives a year at UC San Diego Health.
Across San Diego County, AI is reshaping healthcare. It transcribes audio from appointments and summarizes patient notes. It helps drug companies decode genetic data. It writes draft responses to patient questions. It chats with people with mild cognitive impairments. It even identifies breastfeeding-related conditions from pictures taken with a phone.
All of these enhancements are leading to lasting changes that will dramatically improve medicine, says Dr. Christopher Longhurst, chief medical officer at UC San Diego Health.
“I think the promise is a little overhyped in the next two or three years, but in the next seven to nine years, it’s going to completely change healthcare delivery,” Longhurst adds. “It’s going to be the biggest thing since antibiotics, because it’s going to lift every single doctor to be the best possible doctor and it’s going to empower patients in ways they never have been before.”
These may sound like high ideals, but the money piece of this equation seems to speak to a bright future for AI in healthcare. Investors are taking note of the technology’s promise. According to a recent Rock Health report, a third of the almost $6 billion invested in US digital health startups this year went to companies using AI.
However, all of these innovations come with big questions: Do patients know when AI is being used? Is patient data protected? Will human jobs be replaced? Does anyone really want to talk to a robot about their health? Some worry the technology is progressing so quickly that these concerns will go unaddressed.
“I just hope we don’t get too excited before the technology is really where it needs to be,” says Jillian Tullis, the director of biomedical ethics at University of San Diego. “I’m thinking of Jurassic Park—just because we can do it doesn’t mean we should do it.”
Illustration by Cam Cottrill
The promise—and pitfalls—of AI as a diagnostic tool
Even providers themselves aren’t always keen on utilizing AI programs such as Wardi’s sepsis model.
“Doctors and nurses are usually very, very smart people, and not all of them are going to be excited about having some kind of form of artificial intelligence suggest that someone might be developing sepsis,” Wardi says. “The more senior the physician, the more likely they are not to find value in the model. It could be a generational thing … Younger people are more excited about AI.”
Wardi compares the skepticism around AI to 19th-century physicians’ resistance to the stethoscope. “[Doctors thought] it had no value and would ruin the profession,” he says. “Now, it’s a symbol of medicine.”
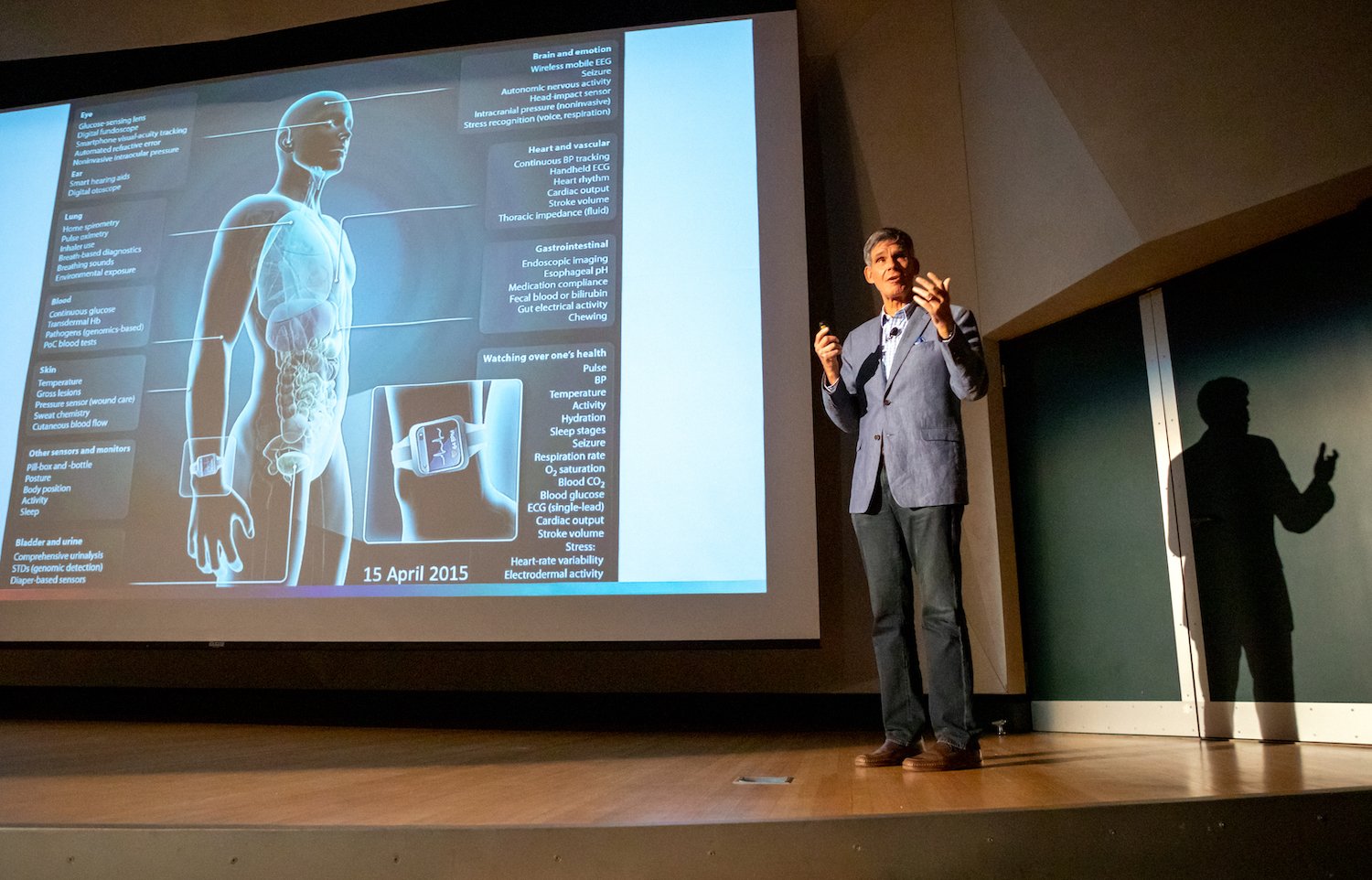
Methods like the sepsis model can be expanded to predict the risk of other diseases, such as cardiovascular conditions, Alzheimer’s, and cancer, says Dr. Eric Topol, director and founder of the Scripps Research Translational Institute.
Courtesy of Scripps Research
“So we take all of a person’s data—that includes their electronic health record, their lab tests, their scans, their genome, their gut microbiome, [and their] sensor data, environmental data, and social determinant data,” he explains. “We can fold that all together and be able to very precisely say this person is at high risk for this particular condition.”
According to Topol, Scripps researchers are even using pictures of the retina to predict Alzheimer’s and Parkinson’s years before any symptoms show up. “Machine eyes or digital eyes can see things that humans will never see,” Topol adds.
Meanwhile, at the San Diego biotech company Illumina, researchers are using an algorithm to analyze genetic information and find mutations that cause disease.
But creating this type of intelligence is a challenge compared to building programs like ChatGPT, which train on data from the internet. Dr. Kyle Farh, VP of Illumina’s Artificial Intelligence Lab, has turned to primates, sequencing their DNA and using that data to train the company’s model, PrimateAI-3D. He hopes to one day use the model to diagnose rare genetic diseases.
Tullis at USD says she’s all for predicting and preventing illness, but she’s worried about the other uses of AI.
“When I read stories about doctors who are fighting with insurance companies about whether or not patients should get certain procedures or treatment, but the insurance company uses an algorithm to make a determination… I get really nervous,” she says.
Diagnosis often requires a human touch, she adds.
“You can look at people’s nail beds; you can look at lumps or rashes in particular ways; you can feel people’s skin if it’s clammy and cold,” she says. “The algorithm can’t do that.”
Illustration by Cam Cottrill
Saving time while protecting patient data
Anyone who’s used an AI model to draft an email or write a cover letter knows it can save a massive amount of time. And doctors and nurses in San Diego are already utilizing AI to take care of some of their more menial tasks.
Several health systems, including Scripps Health, use AI to generate post-exam notes, answer patient questions, and summarize clinical appointments. It can reduce documentation time to “about seven to 10 seconds,” says Shane Thielman, chief information officer at Scripps. “It’s enabled certain physicians to be able to see additional patients in the course of a given shift or day.”
Courtesy of UC San Diego Health
UCSD uses a similar system. According to Longhurst, it’s freed doctors up to focus on patients—not computer screens—during appointments.
“That’s really about rehumanizing the exam room experience,” he says. Since they don’t have to take notes, physicians can make eye contact with patients while the tech transcribes their conversations.
But the approach raises concerns about consent and data privacy. Jeeyun (Sophia) Baik, an assistant professor who researches communication technology at University of San Diego, recently studied loopholes in federal HIPAA law that health data can fall into.
HIPAA does not currently protect health data collected by things like fitness apps or Apple Watches, she says. And that legislative gap “could apply to any emerging use cases of AI in the areas of medicine and healthcare, as well,” Baik adds.
For example, if physicians want to utilize protected health data for any purpose beyond providing healthcare services directly to the patient, they’re supposed to get the patient’s authorization. But it’s debatable whether that applies if healthcare providers start to use the information to train artificial intelligence.
“It can be controversial, in some cases, whether the use of AI aligns with the original purpose of healthcare service provisions the patients initially agreed to,” Baik says. “So there are definitely some gray areas that would merit further clarification and regulations or guidelines from the government.”
A recent California state bill, SB 1120, attempts to clear up those gray areas by requiring health insurers that use artificial intelligence to ensure the tool meets specified safety and equity criteria.
Thielman with Scripps Health says patients must always give consent before the AI tool takes notes on appointments. If a patient declines, providers won’t use the technology. However, “it happens very rarely that we have a patient that doesn’t consent,” he adds.
And, he continues, a human always looks over automated, AI-generated messages answering patient questions. But Scripps doesn’t tell patients that it’s using AI “because we have an appropriate member of the care team doing a formal review and signing off before they release the note,” he says.
It’s the same case at UCSD.
“There’s no button that says, ‘Just send [the message to the patient] now,’” Longhurst explains. “You have to edit the draft if you’re going to use the AI-generated draft. That’s adhering to our principle of accountability.”
Jon McManus, chief data, AI and development officer for Sharp HealthCare, says he realized an internal AI model was necessary to ensure employees and providers didn’t accidentally input patient data into less secure algorithms like ChatGPT. “We were able to block most commercial AI websites from the Sharp Network,” he explains. Instead, his team created a program called SharpAI. It’s used for tasks like summarizing meeting minutes, creating training curriculum, and drafting proposed nutrition plans.
Fixing mistakes—and possibly making them
With artificial intelligence technology, telehealth services could get way more advanced—Jessica de Souza, a graduate student in electrical and computer engineering at UCSD, is currently working on a system that would allow parents experiencing breastfeeding problems to send photos of their breasts to lactation consultants, who could use AI to diagnose what’s wrong. De Souza created a dataset of breast diseases and trained AI to identify patterns that could indicate issues such as nipple trauma.
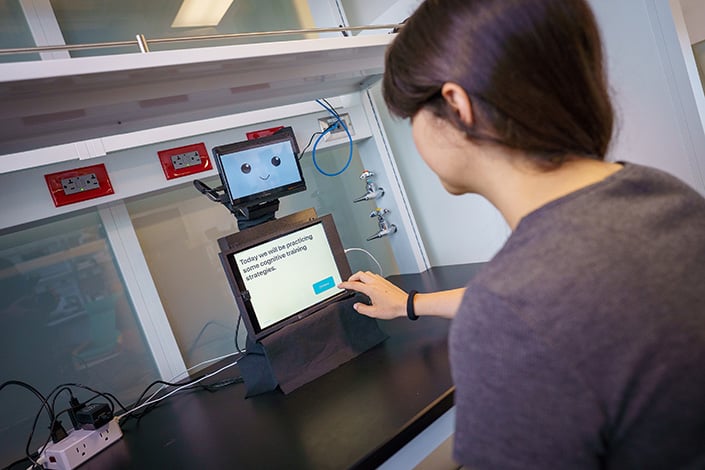
Meanwhile, Laurel Riek, a computer science professor at UCSD, designed a small, tabletop robot called “Cognitively Assistive Robot for Motivation and Neurorehabilitation,” or CARMEN (the name is inspired by Carmen San Diego). CARMEN helps people with mild cognitive impairment improve memory and attention and learn skills to better function at home.
Courtesy of UCSD
“Many [patients] were not able to access care,” she says. “The idea behind CARMEN is that it could help transfer practices from the clinic into the home.”
Uses like these offer another vision for AI in healthcare: to improve patient care by helping doctors assess conditions and find mistakes.
“One of the big things is getting rid of medical errors, which are prevalent,” Topol says. “Each year in the United States, there are 12 million diagnostic medical errors.” According to Topol, those errors cause serious, disabling conditions or death for about 800,000 Americans per year.
He believes that AI can help shrink that number considerably. For example, doctors are utilizing it to review cardiograms, checking if there’s anything a human review missed.
But, Topol cautions, you can’t rely solely on AI. “In anything involving a patient, you don’t want to have the AI promote errors,” he says. “That’s the thing we’re trying to get rid of. So that’s why a human in [the] loop is so important. You don’t let the AI do things on its own. You just integrate that with the oversight of a nurse, doctor, [or] clinician.”
No matter how advanced artificial intelligence programs get, he sees no future where AI would handle diagnosis without human eyes.
“You don’t want to flub that up,” he says. “And patients should demand it.”
Algorithmic bias
An additional hope for AI is that it could correct for implicit racism in medicine, since machines, in theory, don’t see skin color. But the data on which algorithms are built is inherently imperfect.
“The medical bias could be already built into the existing information that’s out there,” Tullis says. “And, if you’re drawing from that information, then the bias is still there. I think that’s a work in progress.”
For example, an AI tool designed to detect breast cancer risk would be trained on previously gathered population data. “But they didn’t get as many Black women as they would like to be included in that data,” Tullis explains. “And then what does that mean for the quality of the data that has been used to maybe make decisions?”
Courtesy of Scripps Research
But there’s bias in every data set, Longhurst says. The key is to choose the right data for the population you’re working with to help address disparities. He points back to the sepsis model. That algorithm, he says, actually performed far better in UCSD’s Hillcrest hospital than in La Jolla.
“Why is that? Well, we tuned the algorithm to identify cases of sepsis that weren’t being picked up [by physicians] until later,” he adds. “We serve different populations in those different emergency departments.”
Patients at the Hillcrest location tend to be younger, which makes it harder to diagnose sepsis early, he says. But the AI algorithm helped to close that gap.
“These tools are going to change healthcare delivery more in the next 10 years than healthcare has changed in the last 50,” Longhurst says. But he hopes the industry doesn’t get ahead of itself—after all, he suggests, what if the FDA approved a new drug for breast cancer and simply said, “It has very few side effects?”
“You’re like, ‘Well, that’s great, but how does it work?’ They’re like, ‘Well, we don’t really know. We don’t have the data,’” he continues. “That’s what’s going on now. It’s like the Wild West. Our argument is that we really need local testing that is focused on real outcomes that matter to patients. That’s it.”
Claire Trageser has been writing for San Diego Magazine for 10 years. She also is a reporter at KPBS and writes for The New York Times, National Geographic, Marie Claire, Elle and Runner's World.
Charitable gatherings, downtown music festivals and theater premieres—of both the heartwarming and thought-provoking variety—are among San Diego’s standout events this weekend. You can’t spell fundraising without ‘fun,’ and both elements are central at Poway OnStage’s Taste of the Towne and the Switchfoot Bro-Am. Listeners of blues, reggae rock and silky smooth jazz can check out the East Village Blues Fest, Field of Dreamz and the San Diego Smooth Jazz Festival, respectively. As for the city’s thespian community, new shows include Cygnet Theatre’s production of Broadway favorite The Spongebob Musical and the world premiere of the OnWord Theatre show Marti Gobel’s Adult Storytime: A Caregiver’s Guide To The Blues.
The tasteful appetizer to Switchfoot Bro-Am’s annual Beach Fest is the laid-back Benefit Party, returning this Thursday from 6-10 p.m. at Viasat. Guests will be treated to a curated dining menu, a performance by Switchfoot with special guests, and the chance to bid on live and silent auction items, including local excursions, apparel packages, and deluxe arts experiences. Individual ticket options include general admission ($300) and reserved seating ($450); the money raised will go towards youth-centered programming at six local nonprofits.
6155 El Camino Real, Carlsbad
Taste of Our Towne at Poway Center for the Performing Arts
June 13
Patrons of Poway OnStage are invited to Taste of Our Towne, the organization’s annual culinary fundraiser, this Saturday at 5 p.m. at Poway Center for the Performing Arts. The evening will begin with auctions, plus bites and libations from over a dozen local vendors before magician Chris Funk, aka The Wonderist, takes the stage for an interactive comedy show.General admission is $115 for Taste of Our Towne; proceeds from this event will benefit Poway OnStage’s Professional Performance Series and Arts in Education Initiative.
Rod Stewart at North Island Credit Union Amphitheatre
June 12
Before (potentially) riding off into the sunset, British rocker Rod Stewart is strutting his stuff stateside with the unconventional voice and unquestionable verve that’s propelled his nearly six decade-long solo career. Though the “Da Ya Think I’m Sexy?” artist’s days on the road may be dwindling, that’s even more reason to give him his flowers in the present. Stewart’s upcoming show this Friday at 7:30 p.m. at North Island Credit Union Amphitheatre will feature prolific singer-songwriter Richard Marx as the opening act. Tickets start at $40.
2050 Entertainment Circle, Chula Vista
Switchfoot Bro-Am Beach Fest
June 13
Following Thursday’s Benefit Party, the 22nd annual Switchfoot Bro-Am will switch (get it?) from its fundraiser to a free day at Moonlight Beach for Saturday’s all-day Beach Fest. From 7 a.m. to 3 p.m. there will be surf competitions—including surf jousting—and from noon to 5 p.m., Sun Room, Telephone Friends, Kimiko, a handful of special guests and, of course, Switchfoot will perform for attendees. Additionally, throughout the day, there will be a variety of vendors and brand activations to explore. Admission is free with RSVP, while VIP pit tickets are $195.
As the mysterious saying goes, ‘If you build it, they will come,’ but instead of Iowa cornfields, this time the message is coming from inside SD’s home ballpark. This Saturday, Ocean Beach natives Slightly Stoopid will headline the first-ever Field of Dreamz Festival, and they’ve brought along a handful of ska, reggae and island-inspired rock acts for the ride. Doors will open at 3 p.m., and fans can see sets by Stephen Marley, Pepper, Sublime—whose first album with frontman Jakob Nowell drops Friday—and more. Ticket options include standard admission ($125), floor tickets ($188), plus All-Star VIP ($244) and Hall of Fame VIP ($610) passes.
Ryan Hardison is a freelance arts and entertainment writer and recent graduate of San Diego State. When he's not staring at his laptop, he's likely eating an adobada burrito or getting sunburnt at the beach.
We love a mega-fancy tasting menu, but let’s be honest—we’re not all blessed with unlimited Wagyu funds. So we picked some of the breakout dishes of the last year (or couple of years) from the best chefs in the city, reverse-engineered their chief charms (salty, smoky, caramelized?) in the test lab of our mouths, and found some budget-friendly alternatives that hit some of the same notes with an everyday price tag.
Where do delicately plucked marigold blossoms adorn Deer Isle scallops, or ingredients like fermented raspberry precede roasted coffee oil, shiro miso caramel, or bronze fennel in a parade of hit-after-hit dishes? Lilo in Carlsbad, of course. San Diego’s newest Michelin star changes its menu with the seasons, but one stalwart dish has kept tongues wagging since opening day last April: the caviar ice cream. A boat-shaped sliver of orgeat ice cream, smoked celery root bushi, and freshly pressed almond oil are topped with a generous heap of caviar. It’s a dish so good and defining that chef Eric Bost will tire of talking about it for a very long time.
Price: $265 for the tasting menu (before tax, tip, and drinks)
Low: S’mores Ice Cream at Stella Jean’s
There’s a reason Stella Jean’s s’mores ice cream is part of the local scoop shop’s “always available” menu. Made with fire-roasted marshmallows and coconut ash ice cream mixed with dark chocolate-covered graham crackers and mini marshmallows, its strangely ashen hue dabbled with flecks of tawny brown is a far cry from the wildly vibrant ube and pandesal toffee flavor seemingly made for Instagram reels. But it’s a sensation in your mouth—smoky, toasty, torched, creamy, marshmallowy, coconutty, ashy, and bitter from the dark chocolate. Pro tip: If you really want to DIY Lilo’s ultra-luxe treat, bring your own caviar.
There’s no question what comes first at Lucien. It’s the egg. Chef and co-owner Elijah Arizmendi’s 12-course tasting menu begins with welcome bites under the calamansi tree before moving inside to start the Journey (the actual name of this section of the menu). The first step is one of the most astounding—a perfectly intact, upright, ochre-hued eggshell containing his take on Japanese chawanmushi (egg custard), topped with a dollop of caviar. The accompanying ingredients have ranged from sweet corn and huitlacoche to banana and buckwheat, but each one has precisely demonstrated Arizmendi’s commitment to French technique with California experimentation and global influence.
Price: $260 for the chef’s tasting menu (before tax, tip, and drinks)
Low: Chawanmushi at Sushi Ota
The biggest difference (besides price) is that while Lucien’s dish changes with the season, Sushi Ota is comfortably predictable. A San Diego staple since 1990, the legendary Sushi Ota has been one of those if you know, you know joints that locals try to keep off the radar. (It hasn’t worked at all.) Known for ultra-fresh fish and ultra-traditional service, the small Pacific Beach restaurant also serves Japanese comfort foods like udon noodle soup alongside sashimi, nigiri, and rolls. But it’s the savory steamed egg custard, called chawanmushi, that really gives you the warm and fuzzies. Add a side of salmon roe (ikura) for a few bucks more, and this dupe is about as good as it gets.
Price: $12 for chawanmushi, $11 for ikura
Courtesy of Chick & Hawk
High: The Birdman Sandwich at Chick & Hawk
Enough ink—and tears, I’m sure—has been spilled over Chick & Hawk’s long and arduous journey to opening its doors. But now that the Encinitas eatery is in full swing, chef Andrew Bachelier’s tightly curated menu of fried chicken sandwiches, fries, and bowls command lines of hungry locals and skate-culture loyalists. The Birdman, the signature hot chicken sandwich named for partner and skateboarding legend Tony Hawk, is piled with cabbage slaw and pickles and slathered with a tangy kimchi comeback sauce on a soft brioche bun. Although this Nashville meets California meets Mississippi meets Korea sando doesn’t command a triple-digit price tag, the fact that it’s nearly a $20 chicken sandwich (sans side) has been a topic of conversation. Bachelier—who worked at Addison before opening Jeune et Jolie, then launched SDM’s 2024 “Best New Restaurant,” Atelier Manna—and his team earned that price tag.
Low: 5-Piece Korean Fried Wings at Cross Street Chicken & Beer
It’s hard to beat Koreans at the chicken game. Korean fried wings are defined by a double-fry technique—first at a low temperature to ensure the chicken is cooked through, then at a high temperature to ensure the famed extra-crispy, ear-splittingly crunchrageous magic. At Cross Street, they follow a similar fusion ethos as Chick & Hawk, using inspiration from the American South as well as Thailand, Korea, Vietnam, and more, with flavors like “Seoul Spicy” or “Honey Butter” for whatever you’re feeling that day. Pair it with a cold beer to go full chimaek (a popular Korean combination of pairing fried chicken and beer). Now that’s a combo—and price tag—that’s hard to beat.
Price: $8.75 for five wings
Courtesy of Trust Restaurant Group
High: Steak Frites at À L’ouest
PB&J. Captain & Tennille. Brad Wise and steak. Steak frites ranks among the iconic global duos. And when the holy union of prime cuts and twice-fried carbs comes from Wise and the meat-loving masters at Trust Restaurant Group, it’s a pretty safe bet. À L’ouest—the group’s newest fancy, but not fussy, drippy plant dreamscape of a French steakhouse on the prime corner of 30th and University in North Park—gives guests a choice: 12-ounce New York strip, 8-ounce filet mignon, or 8-ounce Wagyu hanger, topped with sauce au poivre (the classic French pan sauce—peppercorns, shallots, heavy cream, brandy) and served with a heaping pile of 24-hour salt-brined fries and a watercress salad. One bite acts as a transport to a Parisian brasserie, so if you think about the cost in terms of time-space travel, it’s a pretty great deal.
Price: starts at $48
Low: Shepherd’s Pie at The Shakespeare Pub & Grille
To satisfy the same urge for meat and potatoes, feel at least moderately European while doing so, and save a couple quid, a trip to The Shakespeare in Mission Hills ticks all the boxes. The classic British shepherd’s pie arrives in a piping hot oval au gratin dish, smothered with a thick layer of mashed potatoes. Beneath it lies a hefty portion of marinated ground beef and vegetables in the pub’s secret sauce, and while there are a few choices of sides, the correct order is peas and “proper” chips (a.k.a. chunky, thick-cut fries versus the typically thinner American “French” fries). It’s more tickety-boo than très bien, but it’s immensely satisfying in any language.
Beth Demmon is an award-winning writer and podcaster whose work regularly appears in national outlets and San Diego Magazine. Her first book, The Beer Lover's Guide to Cider, is now available. Find out more on bethdemmon.com.
Chefs have done gobs of thankless, lumbar-breaking work over years to land the role. Restaurateurs put their entire livelihoods on the line, microdosed sleep, took ultimate responsibility for every minor stress. They earned the spotlight they get. But ask one of them, and they almost always defer to a line cook who’s showed up for years, been deep in the thing, and whose absence would bring the kitchen to its knees. Or the bartender with a warmth that draws people whether they’re thirsty or not. Or the noble and spreadsheetable soul in charge of purchasing everything needed for the nightly show.
Roger Feria Krile is not only the guy you want to be friends with at work, but also the guy you want to hire: respectful, nose-to-the-grindstone, versatile. And he’ll drop off a fresh batch of cinnamon rolls at your house for the holidays. Born in Tijuana, Krile moved to the US with his mom and sister when he was in elementary school. He saw the sacrifices his mother made to give her children a better life, and he pushed himself to live up to that brighter future.
He came to cooking during the pandemic, asking himself, “What do I really love to do?” His answer: “Bake cakes for friends and break bread with people,” he says. That led to a culinary school degree and a stint in a Michelin-starred NYC kitchen, where he grew to “love and understand” fine dining. Now back in San Diego, Krile’s showing up at Animae in a major way. He does prep work three mornings a week and comes later in the day twice a week for dinner service. Most line cooks do one or the other, but he requested both tours of duty.
“Gotta get my reps, keep my skills sharp,” Krile says, “and I don’t want to miss the rush.” Prep work in the mornings helps him learn how Executive Chef Tara Monsod uses each ingredient to the fullest. Krile’s not just a line cook. One-quarter Filipino (and learning about his culinary heritage from mentor Monsod), he’s building his own Mexican-Filipino pop-up concept. Look for Sarsa—Filipino for salsa—where every dish is a play on words fusing Mexican and Philippine Spanish or Tagalog. He’s already R&D’d a breakfast sandwich, the tortantalong: a torta filled with a signature Filipino eggplant omelette called a tortang talong. Friends in the industry say it’s unexpectedly delicious.
“He shows up every day with a clear goal of one day opening his own restaurant, and that drive pushes him to go above and beyond,” says Monsod. “He is constantly learning, asking questions, and absorbing as much as possible, all while leading by example on the line.”
Photo Credit: Matt Furman
Ruben Martinez
Purchasing Manager, Mister A’s
Ruben Martinez knows every bottle of wine at Mister A’s—not necessarily by taste (though he was on the tasting committee for years), but by where they are in storage and whether they need replenishment. Owner Ryan Thorsen wants the wine list at 100 percent available every night, and Martinez’s job is to make that a reality. He’s been keeping inventory on Mister A’s wines since the 1970s, back when he worked for founder John Alessio. And it’s not just vino: Martinez also procures the ingredients, arriving at 5 a.m. to meet delivery trucks, stock shelves, and alert chefs if anything’s amiss.
Then he hits the dining room for a once- or twice-over to find any imperfections. If a light is out, if the plumbing acts up, if something major happens after he leaves in the afternoon, he’ll fix it all. He’s the best guy to ask, anyway; he knows every inch of Mister A’s. “Before ‘Google it,’ there was ‘Call Ruben,’” Thorsen says.
Martinez started out in hospitality at 17 with his father at Hotel Del. “I thought it would be easy working with my dad,” he says. “But early on, he caught me fooling around with the boys and told me, ‘We’re here to make money for the company. If you’re not willing to work, get out of here.’” That set him straight and set the foundation for Martinez’s lifelong dependability.
He moved to Mister A’s a couple years later, and after over five decades, he’s now the indispensable purchasing manager who worked with Alessio, Betrand Hug, and now Thorsen. Later this year, he’s planning on retiring—though he’s already offered to keep showing up a couple days a week and help out with Thorsen’s new project at Liberty Station.
Thorsen knows this man is a gem. “I don’t think we fully grasp what it will feel like without him,” he says. Last year, he threw Martinez a surprise birthday party in Mister A’s Blue Room, inviting Martinez’s family and a whole cast of coworkers going back to Alessio days. Martinez says he had to leave the room to hide his tears.
Photo Credit: Matt Furman
Patrick Mattoon
Lead Prep Cook, Ironside Fish and Oyster
There’s an hour most people never see, when a restaurant’s technically awake but not yet accountable, and that’s where Patrick Mattoon lives. He’s been the foundation of Ironside’s prep team for the past five years, quietly guiding the day toward success. He and his team are the first in, and they turn on ovens, check deliveries, catch mistakes before they become problems, and fix everything without ceremony so the chefs and line cooks walk into a day that already works.
Mattoon organizes, but more importantly, he owns. There’s no job too small, no detail beneath notice. In a kitchen, bad prep’s the one thing you can’t fix later, no matter how talented of a chef is at the helm.
Five years in, Mattoon still approaches each day with the same care and intensity that he had on day one. He takes every task seriously and sees it through completely—the kind of consistent work that doesn’t draw attention but makes everything else possible. When the restaurant got a soft serve machine, a notorious maintenance nightmare, he taught himself how to clean and run it just to make sure it never broke, not for credit but because that’s just how he’s wired.
“He is a silent leader who has the respect of the entire team due to leading by example,” says Ironside chef Jason McLeod.
Photo Credit: Matt Furman
Arturo Celestino
Lead Line Cook, A.R. Valentien at the Lodge at Torrey Pines
Through 23 years, three executive chefs, and a recent kitchen remodel, lead line cook Arturo Celestino is a constant at A.R. Valentien. He’s there at 6:30 a.m. five days a week—sometimes six—for the Lodge’s breakfast service. That means he’s up early prepping potatoes, slicing mushrooms, whisking pancake batter, and stirring sauces “always with a smile,” says Owen Beatty, the restaurant’s new chef de cuisine. “He’s a good leader.”
Celestino shows the younger guys how to make the eggs fluffy, so the omelettes are always perfect (don’t stop twirling the spatula!). He keeps his line in line when their spirits start to naturally droop during the morning shift home stretch when his crew just wants to get out of there. As the lead, he’s also the one chefs turn to when newbies need motivation.
His secret sauce: “mucho talking!” It keeps people happy, and it also helps the chefs retain talent in the kitchen.
Celestino learned to cook out of “necesidad,” he says. He cut his teeth on fine dining at Pacifica Del Mar at the Hyatt and moved to A.R. Valentien in 2003, just a few months after it opened in 2002.
“I’ve had good jefes,” Celestino says of the three executive chefs he’s known at A.R. Valentien: Jeff Jackson, Kelli Crosson, and now Michelin-starred Eric Sakai. Under Jackson—who’s known for pioneering farm-to-table dining in San Diego—Arturo learned to appreciate local ingredients.
“My favorite is basil,” he says, “added to tomato sauce with garlic, it’s mmm.” Fresh basil plays the supporting role in A.R. Valentien’s signature brunch plate, which is also Celestino’s top choice on the menu (to make and to eat), via the Bull’s Eyes: slow-roasted eggplant with sunny-side-up eggs, tomato sauce, and La Quercia prosciutto.
“I love my job,” Celestino says as he flashes that smile. “It’s not just a plate of food. It’s an experience.”
Photo Credit: Matt Furman
Tony Suarez
Bartender, The Marine Room
If you’ve been to The Marine Room, you’ve probably met bartender Tony Suarez. With his charming Cuban accent and dapper vest and tie, he makes it his business to regale guests coming and going—even while he’s pouring, mixing, shaking, polishing glasses, and taking orders.
“Over 90 percent of our guests are celebrating a special occasion,” he says. “So I keep up the celebration throughout their whole visit.” He’ll make you a sparkling toast and a customized cocktail, and on your way out, he’ll wish you a happy birthday (again) and invite you back for drinks on him.
“My goal is always to delight the guest,” he says. “I like to discover how you feel and lead you to what you would like to drink.” That spirit of experimentation has led to new signature cocktails, such as the Gerald—crafted for a neighbor who’s a regular—featuring housemade pomegranate puree and bourbon, or the I Drink of You with local Bebemos tequila, Gran Marnier, and Green Chartreuse. You won’t find this anywhere else.
“[Suarez] has mastered the art of the personalized guest experience,” says Marine Room’s Executive Chef Ananda Bareño. “He remembers the small details and favorite orders that make our regulars feel like family.”
Suarez’s tenure at the Marine Room started with a walk on the beach and a knock on the door. He was impressed by the beautiful location, and he asked if they were hiring. He immediately started as a server assistant—right before Valentine’s Day. The bartender took Suarez under his wing, and he took to the books to learn all about spirits.
He’s taken on the bartender role with wisdom and grace, offering a sympathetic ear, a pick-me-up, and a “human to human connection,” he says. Ten years into his career, the surroundings still inspire him as much as they did on day one.
“The Marine Room, the windows onto the ocean, [all] have a healing effect,” he says.
Kelly H. Harfouche, founder of KQ Aesthetic Society, knows firsthand that cosmetic treatments like fillers, neurotoxins, and microneedling, can not only enhance a person’s appearance and restore confidence, they have the power to truly change a person’s life. An expert injector has the ability to tailor treatments to each individual patient’s anatomy and goals for personalized results. Harfouche, a board-certified nurse practitioner, has spent nearly a decade perfecting her craft as an aesthetic injector and integrating her multifaceted artistic skills with precision patient care. Her commitment to continual education and training, plus a passion for helping people look—and feel—their best, set KQ Aesthetic Society apart in a sea of local medspas.
For many people considering nonsurgical treatments, the intent is to look refreshed and refined. KQ Aesthetic Society’s philosophy eschews a cookie cutter approach that bases treatments around units, instead working to understand each person’s unique goals, then curating a treatment plan to fit that vision. Harfouche focuses on “inclusive luxury,” the belief that everyone deserves access to aesthetic treatments, respective of budget restrictions. She develops long-standing trusted relationships with her patients, and works with each one to achieve their aesthetic objectives and address the underlying causes of their concerns.
“For me, forming an honest and open relationship with every patient who walks through the door is essential. This means understanding them on a deeper level and meeting them where they are to define and achieve their individual goals,” she says.
Drawing on her artistic background, which inspired her transition into medical aesthetics, Harfouche sees each client as a “unique canvas.” Rather than relying on standardized procedures, the practitioner’s distinctive approach combines her profound understanding of the physiological and anatomical changes associated with aging with an unwavering commitment to ongoing education about the newest products and their mechanisms of action. Her goal is to make each patient feel beautiful in their own skin and to embrace their individuality.
She has also pioneered a way to combine her talent for aesthetic artistry with her philanthropic nature. Harfouche is one of only a handful of providers using dermal fillers to treat patients with lip asymmetry and scarring resulting from cleft lip surgery. Patients travel from around the country for this transformative treatment, noting increased confidence and a restored identity. She hopes to eventually launch a training program to help fill the void in this space.
“My passion has always been connecting with people and giving back in any capacity that I can,” she says. In the rapidly advancing landscape of aesthetic medicine, you can place your confidence in Harfouche and KQ Aesthetic Society to deliver exceptional care. To learn more or book a consultation, please visit kqaestheticsociety.com.
His ascent has been stealth and humble, which fits the man. When Liberty Station was struggling to convince people it existed over a decade ago, Sicilian chef Accursio Lota’s food at Solare Ristorante was a tractor beam for food people who sniff out hidden talent like truffle dogs. In 2017, he won the World Pasta Championship (a legit competition from global pasta brand Barilla) and struck out on his own, opening his and his wife’s from-scratch pasta trattoria in North Park (Cori Pastificio). Gambero Rosso—the Italian version of Michelin, the most respected source—has clamored for the restaurant since it opened, naming it “New Opening of the Year” and this year giving it their highest award, “Tre Forchette” (Three Forks), only knighted on a handful of US restaurants.
So this year, Lota opened his grandest thing—Dora Ristorante—and it pulls everything together. Steps from San Diego’s world-class theater, La Jolla Playhouse, it’s laden with brass and large-format murals, tile work and mosaics—like the one on the wood-burning oven that blisters, chars, and smokes a good portion of the menu. Their housemade focaccia is a new street drug (try it with the puttanesca, his grandmother Dora’s recipe). The olive oil-cured sardines make “sustainable seafood” and ethics not taste like a compromise. Dora might finally be the one to solve the “where do I eat before the world premiere at LJP” dilemma.
The yuzu-colored building that helped build North Park’s modern food culture is alive again. Years ago, the ornate French Quarter–inspired spot on 30th Street was home to chef Matt Gordon’s Urban Solace (duck macaroni and cheese). Then it laid conspicuous and fallow until a few months ago when Bacari took it on. It’s an LA transplant, but they’re proving forgivable of that trespass. Chef and co-founder Lior Hillel cooked at Jean-Georges before opening the first of this Venetian-style restaurant in 2008 with brothers Danny and Robert Kronfi (Bobby started his food venture with a pop-up dinner series in his college apartment at USC).
For dinner, it’s house-baked bread, crudo and shrimp ceviches, Mediterranean street corn, lamb hummus, shawarma, and glazed pork belly. Weekend brunch is bellinis and French toast and burekas (famed Jewish stuffed puff pastry), and chef Noa’s cauliflower (caramelized with chipotle). It’s Italian-ish with a heavy dose of pan-Mediterranean and Middle Eastern. Doesn’t hurt that they left the iconic exterior as is, adding chandelier-farmhouse insides with charm that echoes two of the city’s dearly departed (Jayne’s Gastropub, Cafe Chloe).
Courtesy of TRUST Restaurant Group
À L’ouest
Much tolerance for friends who hate mussels because they look too biological. But if they manage to dislike À L’ouest’s—served over ice with vadouvan curry aioli and chili crisp—then you’ve successfully identified your brokemouth friend and should try bicycling or crafting with them to bond instead of eating in public places. It should be on everyone’s short list for dish of the year.
Chef Brad Wise and his team have earned their rep over multiple concepts—Trust, Fort Oak, Cardellino, Wise Ox, Rare Society. But he’s been eyeing this corner of North Park since before he opened his first (Trust, in 2016). North Park has been rising for a while, and À L’ouest feels like the missing piece—an indoor-outdoor brasserie stunner on the marquee spot of 30th and University, which long sat boarded up and vacant like a neighborhood missing a front tooth.
As with his other concepts, woodpile is king; smoldering red oak boosts the flavor of just about everything. Get the spätzle with braised rabbit, maitake mushroom, secret de compostelle (the famed Basque sheep’s milk cheese), and black truffle. Or the chicken liver parfait with persimmon, fennel aigre-doux (sweet-sour), and chives on toast. Or, like everyone else in there—the steak frites.
Photo Credit: Eric Wolfinger
Fleurette
Chef Travis Swikard’s first solo restaurant, Callie in East Village, proved how details can make the most composed of us blubber a little in fine places—from citrus left in ovens overnight to blacken and transform, to the Scripps Oceanographic Institute saltwater he keeps his spot prawns thriving in until ordered, to the days-long fermentation and stone-ground dukkah that turn carrot shavings into a statement piece.
Now, he’s focusing on French food with a fitter, less buttery San Diego heart. Fleurette is his doubling-down, a SoCal riff on the food he learned under mentors Daniel Boulud and Gavin Kaysen. The French gave us the mother sauces, and Fleurette showcases the lightest and brightest evolutions. Like the anchoïade on his beef tartare, which uses famed Italian anchovy sauce colatura di alici, mixed with cured egg yolks over tiny, uniform-sized cubes of raw, USDA Prime Flannery beef.
There is soubise (onion sauce), a sauce vierge (tomatoes and herbs), and a fennel marmalade on the duck liver and bone marrow pâté. Although the structure is stunningly pure glass, Fleurette’s in a location—an office park on the edge of La Jolla, near UTC—that few chefs would be able to pull off. But Swikard’s Michelin-bound house of saucework pulls hard.
The Escondido taqueria from Rosarito-born-and-trained chef Juan González and farmer Megan Strom took the county by storm this year. The married couple started as a popup four years ago, hosting farmside dinners before taking up residency at Vino Carta in Solana Beach. Strom was working a small, 5-acre heirloom bean farm in Valley Center owned by Mike Reeske (aka “The Bean Man”) when he retired and sold them the plot.
The huge bonus was that the sale included Reeske’s famed collection of beans, curated over 20 years. The couple planted other things and now grow much of what they serve in the form of tacos and burritos at a permanent spot in Escondido: Mesa Agrícola.
The menu’s bone simple: housemade tortillas in your choice of taco or burrito norteños (which are smaller, like burritos de hielera) that change constantly and often topped with guisados (Mexican braises or stews) like lamb and garbanzo, birria, chicharrón, mushrooms al ajillo, rajas, you name it. And, of course, some of the best beans honoring the local legend of Reeske.
Courtesy of Lucien
Lucien
San Diego is now the recipient of national food buzz. The dark ages—during which we learned how to sear ahi and asada some carne and called it a day—felt prolonged, and they were. The problem was never ingredients. San Diego County always had the best raw dinner materials (more small farms per capita than any county in the US, seafood right there); it just didn’t have a critical mass of highly trained chefs to do them justice. Easy to understand the chef dearth.
For a very long time, if you wanted to be a serious chef you had to go to the restaurant superplexes of New York, San Francisco, or Chicago (which imported their raw ingredients from places like San Diego). But now—credit farmers or Alice Waters or Dan Barber or Michael Pollain or the reasonable conclusion that food picked right here tastes better than food picked way over there—some of the most talented chefs are moving to the ingredients, not the other way around.
In San Diego, we got Richard Blais, Swikard, and now Elijah Arizmendi, who cut his teeth in Vegas with Joel Robuchon (plus Boulud and Thomas Keller) and was chef de cuisine at NYC’s L’abeille when it got its first Michelin star. His debut restaurant in La Jolla—with partners Brian Hung and Melissa Yang—is a dark, moody multicourse tasting-menu hideaway with one of the best egg dishes in the city.
Troy Johnson is the magazine’s award-winning food writer and humorist, and a long-standing expert on Food Network. His work has been featured on NatGeo, Travel Channel, NPR, and in Food Matters, a textbook of the best American food writing.
There’s a creative inertia that resides in San Diego, producing a near-constant stream of cool events. Fortunately, this weekend is no different. Those with an artistic inkling can search for inspiration at MCASD’s EXPO Design Market or admire the mixture of live performance and neighborhood charm during the North Park Music Fest. Foodies can dine (with wine) at Stake Chophouse & Bar during its ZD Wines Dinner or explore Barrio Logan’s standout eats at the Sabor Del Barrio. Plus, Pride Month is already in full swing in SD with the return of DISCO RIOT’s Queer Mvmnt Fest and the two-day Out & Abt Music Festival.
Stake Chophouse & Bar is collaborating with Napa Valley’s ZD Wines—a family-run winemaking institution that’s been around since 1969—on an intimate four-course dinner this Thursday at 6:30 p.m. Throughout the meal, each dish will be paired with a curated pour from ZD Wines, with patrons set to receive a chardonnay, pinot noir, and pair of cabernet sauvignons. Dinner guests will also be treated to insight on the night’s wine pairings from ZD Wines’ senior winemaker Chris Pisani. Reservations are $210 pre-paid through OpenTable.
Take advantage of all the dynamic attractions that the Barrio Logan Cultural District has to offer—and eat very well while you’re at it—during the third annual Sabor Del Barrio. This Sunday from noon to 4 p.m. attendees can devour their way through 35 neighborhood staples and traverse the tasting stops on foot, by bike, via a free trolley shuttle, or a combination of the three. Tickets are $40 online ($55 day of) and come with complimentary admission to Quint Gallery, the Athenaeum Art Center, and the Chicano Park Museum & Cultural Center, plus a free tour of Tao of Clay.
Sam Hinton Folk Heritage Festival at Old Poway Park
June 6
Survey the depth of oral storytelling during the free annual Sam Hinton Folk Heritage Festival this Saturday from 10 a.m. to 4 p.m. at Old Poway Park. Named for harmonica virtuoso, marine biologist, and longtime San Diegan Sam Hinton, this event highlights folk artists who specialize in time-honored traditions. Throughout the day, attendees can see performances by musicians with roots in Americana, Cajun, and Appalachian rhythms on the main stage, dance in the Templars Hall, and hear historical tales from the Storytellers of San Diego in the Porter House.
14134 Midland Road, Poway
North Park Music Fest
June 6
Psychedelic rockers Frankie and the Witch Fingers will headline an eclectic lineup at the North Park Music Fest. This Saturday, enjoy sets from noon to 1:45 a.m. from over thirty performers—including DJs, bands, and local acts—across a dozen North Park venues. Ticket options include general admission ($25 online, $35 day of) and VIP passes ($65) which come with lounge access at Granada House, line-skipping privileges and more; festival proceeds will go towards the North Park Business & Neighborhood Foundation. Plus, performances at Pure Pawsh, Visual Art + Supply, Overland, and Playground Art + Coffee will be open to the public.
North Park
Out & Abt Music Festival
June 6 & 7
The calendar has just flipped to Pride Month, and Out & Abt is celebrating in style. The two-day Out & Abt Music Festival begins Saturday from 3-10 p.m. at The Soap Factory with drag shows, circus acts, a manic pixie dream market, two stages of live music, and last but not least, a mechanical bull. The festivities will continue with an after party from 10 p.m. to 2 a.m. at Gossip Grill and conclude with an afternoon pool party at Hard Rock Hotel San Diego on Sunday from 1-7 p.m. Ticket options include weekend general admission passes ($70), and entry to the music festival ($30), after party ($17) and pool party ($27).
Citywide
Photo Credit: Kevin Berne
Theater & Art Exhibits in San Diego This Weekend
The Monsters at La Jolla Playhouse
June 2-28
Fresh off its Drama Desk Award-winning run in the Big Apple this past winter, The Monsters will have its first West Coast production beginning Tuesday in the Mandall Weiss Forum at La Jolla Playhouse. Written by and co-starring Ngozi Anyanwu, The Monsters finds its reconciliatory narrative in a young woman yearning to repair her relationship with her estranged older brother in the brutal and unforgiving world of mixed martial arts. The Monsters will have preview performances this Tuesday through Thursday at 7:30 p.m., Saturday at 2 & 8 p.m. and Sunday at 1 & 7 p.m., with tickets ranging from $30-$74.
Ryan Hardison is a freelance arts and entertainment writer and recent graduate of San Diego State. When he's not staring at his laptop, he's likely eating an adobada burrito or getting sunburnt at the beach.
AVRP Studios’ tradition for Design Excellence and Innovation began in 1976 with Doug Austin, FAIA, in Solana Beach, California. The firm has since grown to complete major projects throughout the United States and Canada. We think of ourselves as a family and we care deeply about people. We want to inspire, help make their lives richer and more complete through our efforts. We believe that architecture is one of the most important art forms because of the impact it can have on the lives of those it touches. We’re delighted to have been recognized with over 150 awards for design excellence.
703 16th Street, Suite 200, San Diego, California 92101 | 619-704-2700 | avrpstudios.com